Ebola Virus Disease Outbreaks in West Africa 2014 – 15: Multi-stakeholder responses to a complex crisis
This article was authored by David Nabarro. It was first published on 02 June 2025 .
During 2014, the numbers of people diagnosed with Ebola Virus Disease in West Africa was doubling every three weeks. The Presidents of the most affected nations (Guinea, Liberia and Sierra Leone) sought international support for combating the outbreaks, and the United Nations (UN) system was asked to help.
The 2014-15 outbreak of Ebola Virus Disease in West Africa started in the interior of Guinea, West Africa, in December 2013 probably as a result of contacts between a child and a bat. The virus is contagious, spread through contact with people’s body fluids. But the outbreak was relatively localised for several months. In May 2014 the President of Guinea visited the World Health Assembly in Geneva. He assessed that relatively few cases had been reported in his country and that the outbreak was under control. At that time his country was negotiating a deal with an international corporation to create a new mining operation in the interior of the country.
Medecins sans Frontieres was ringing the alarm bells about the outbreak in Guinea in April 2014 and was concerned that the World Health Organisation (WHO) was not taking its reports seriously. Was the WHO influenced by the position of the national government who were understandably anxious that this outbreak might have severe economic consequences for the country?
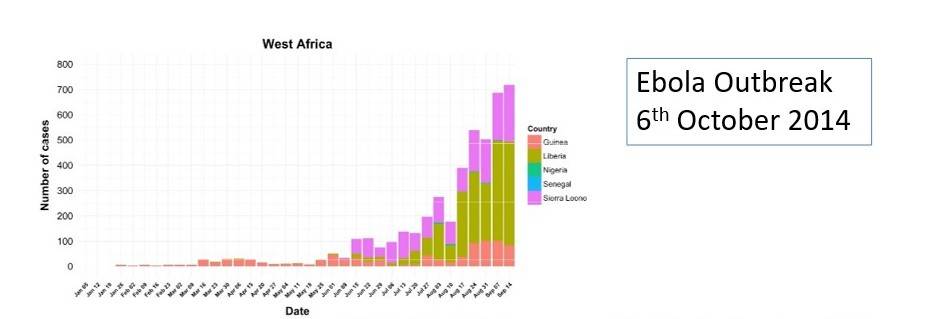
During June 2014, reports started to come through that large numbers of people were becoming ill with Ebola in Liberia and Sierra Leone: many of these were health care professionals. Severe illness was spreading in urban areas of all three countries (Guinea, Sierra Leone and Liberia), with numbers of cases doubling in less than a month.
David Nabarro’s first task was to assemble information about the extent of the challenges posed by the disease and then recommend optimal ways in which the Secretary-General’s office could help. This involved making sense of the many different perspectives at the time on what was going on and what needed to be done. David sought efficient ways to listen to these perspectives and make sense of them. These emerged from visits to the affected countries, to WHO, other UN entities, the World Bank, the African Development Bank and African Union, as well as to Washington, Paris, London, Brussels, and (later) Nigeria and Mali. There were also frequent exchanges with country representatives in the UN General Assembly and Security Council. In the early weeks David was trying to establish a meaningful pattern while being open to everyone’s point of view in a rapidly evolving situation. That meant moving quickly between having a detailed impression of specific needs and – at the same time – a meaningful big picture of the outbreaks, often doing this several times a day.
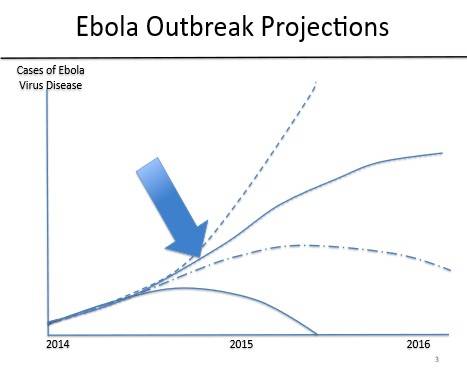
The thinking in August 2014 was that the scale of the outbreak was unprecedented with the disease spreading in urban areas and no clarity on the chains of transmission and the origins of each person’s infection. Around half those who became ill went on to die: the hospitals in the three affected countries were overloaded and there was increasing concern among the local population that hospitals were not safe places to be. The priority was to reduce the mortality rate and slow the rate of spread – ie to bend the outbreak curve – before getting into the more conventional approach to infectious disease control – finding cases, isolating them, tracing contacts and containing surges.
Access to Treatment: During David’s August 2014 visit to the region there were requests from the Presidents for specially constructed Ebola Treatment Centres where the emphasis could be on saving lives, limiting the spread of the virus, and enabling health care workers to stay safe.
Behaviour change to reduce risks: Most importantly, the in-country view was that there should be sharing of up-to-date information, with the local populations, about actions they could take to reduce their risks of being infected. This was a strong position taken by Ellen Sirleaf Johnson, Liberia’s president, and she encouraged Members of Parliament from each county to take the initiative. In Liberia, the leader of a long-term UN Peacekeeping Mission (Dr Karen Landgren) had, since early 2014, been working with the President, engaging at county level, encouraging local leaders to be confident in advocating behaviours that reduce spread of the disease.
During August, David worked closely with public health experts from national governments, WHO, UNICEF, and many providers of assistance, together with logistical specialists who were generously made available by the World Food Programme. There was widespread appreciation of the need for a dramatic leap in response capacity throughout the most affected countries because of the exponential increase in the number of cases.
The emerging plan (see figure 4) identified five priorities:
There were 13 mission-critical actions identified through the conversations. These included:
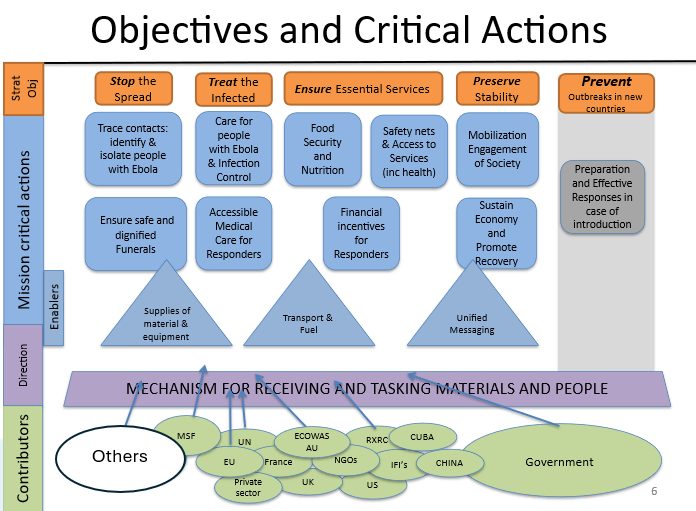
To ensure there was adequate response capacity in Ebola-affected countries, attention was given to building in-country platforms to support responses. These platforms were needed to prioritize and facilitate more ambitious action for behaviour change, to increase the number of accessible beds for patient care, and to encourage safe and dignified burials in the event of death.
The emphasis on behaviour change called for implementation of massive sensitisation campaigns about the extremely infectious nature of Ebola disease and the benefits of adopting behaviours that reduce intensity of transmission, including the immediate isolation of people who are suspected of having the disease.
More beds were needed, so the Presidents requested help with establishing new 50-person Ebola Treatment Centres to be located close to where people lived. In August 2014, the expectation was that to have adequate capacity, at least 20 new Treatment Centres would be needed.
And a programme was established for the safe and dignified burial of those who died had to be instituted.
So, the strategy for the early months was focused on 3B’s: Beds, Burials and Behaviour change.
The leaders of the three most affected countries contacted the UN S-G seeking support at the end of July 2014. When David Nabarro met with them in August, they all conveyed a sense that their needs had been neglected by the rest of the world. They noted that passenger and freight traffic to the region had greatly reduced (Royal Air Morocco was an exception), personnel from diplomatic missions were seeking to leave, and businesses were scaling back on their ambitions.
Because of the economic impact, the World Bank was involved. The President at the time, Dr Jim Kim, was an infectious disease specialist who became engaged in the effort to accelerate the response.
The working environment was difficult and stressful. There were reports of response teams being attacked as they sought ways to bring help to some interior villages. From the UN side, the World Food Programme (WFP) provided logistics support for platforms in the form of transportation, construction, warehousing and land- and air-corridors (operating rotary and wing aircraft) between and within countries. The World Food Programme’s air transport linking the three countries often encountered challenges: its planes could not land in Senegal until the outbreak appeared to be coming under control.
In September 2014, the UN General Assembly established the UN Mission for Emergency Ebola Response (UNMEER) as the first ever UN public health Mission. UNMEER offered leadership, high-level coordination, response platforms and senior response officers in each of the affected countries. UNMEER was led by Tony Banbury, Special Representative of the UN S-G, from a base in Accra. The UNMEER strategy was to align the national governments’ and UN system’s responses to Ebola, to establish national emergency response centres in each country and to increase response capacity in local government areas (Districts in Sierra Leone, Counties in Liberia and Prefectures in Guinea). This form of networked multi-level leadership enabled responders to collaborate and quickly adapt to a shift in the pattern of emerging cases.
UNMEER drew on the WHO strategy for immediate actions to reduce the intensity of the Ebola outbreaks in the affected communities to a stage where chains of transmission could be understood and the disease could be fully contained.
Space was needed for dialogue, sharing experiences and encouraging alignment of approach among national government Ebola emergency response teams, government staff, in-country partners, non-governmental organizations, religious groups, businesses, and leaders and teams from UNMEER, WHO and across the UN system. In September 2014, the Special Envoy established a Global Ebola Response Coalition (GERC) designed to enable strategic updates to be shared, and tactical priorities to be discussed. More than 100 responder groups were working in the region: the GERC contributed to their coordination in the face of an outbreak that was advancing in ways that were hard to predict.
The GERC welcomed any responder organization, including those who were not comfortable with the UN’s approach. The GERC meetings took place every week (Fridays) with participants speaking in English and French. The utility of the GERC depended on the strong strategic engagement leadership of WHO, UNMEER, UNICEF, WFP, other UN system actors, and the constant engagement of Medecins Sans Frontieres, the Red Cross movement and many other national, regional and international NGOs.
The GERC, the national emergency management offices and the coordination capacities at district or county levels, equipped responders to anticipate and adapt to changes in the pattern of spread.
Towards the end of 2014, the focus shifted from emergency efforts to take the steam out of the outbreak to a steadier state where there was the capacity to detect new cases, identify contacts, work out chains of transmission and keep a lookout for new surges (as took place in Western Sierra Leone in 2015). Development assistance agencies, philanthropies, and pooled funds were all called on to support different phases of the response and benefited from the co-ordination offered through the GERC. The GERC also offered a space where responder organizations could come together and consider whether they were getting the upper hand in the fight against Ebola. There was plenty of space for national actors whose participation was greatly appreciated: they were seen as a valued source of constructive energy.
It became clear during 2014 that there were high levels of public concern in West Africa about the dangers of Ebola for individuals and societies, and the challenges of ensuring a collaborative response. There were questions in the GERC about how best to do this. UNMEER engaged anthropologists from the region and tasked them to provide advice on optimal ways to engage with local communities. They suggested that personnel should not go to the villages wearing jackets adorned with the logos of different responder organizations and accompanied by military escorts. This meant they were more likely to be targeted. Instead, the connection should be low-key, with a small gift to the local chief and a respectful exchange emphasising that the disease is caused by a pathogen and that the pathogen, not the people themselves, is the problem. In the first encounter, the role of people as partners in the response would be emphasised, and leaders would be invited to suggest how their key role could be enhanced. The role of people as partners in the response was championed by the President of Liberia in August 2014: she requested that any efforts to control quarantined populations should not be accompanied use of lethal force.
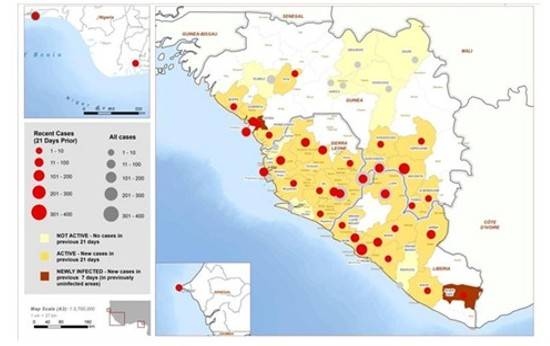
As the outbreaks continued into 2015, and the disease was confined to, and still active in, a smaller number of areas. In other areas the outbreak was quieter but there was still the potential for resurgence. This meant that the strategic focus shifted to finding cases – identifying and acting promptly in case people are suspected of being newly infected, as well as on tracing contacts of anyone who might be newly infected and encouraging greater community engagement in all aspects of prevention, surveillance and response.
The strategic shift was from reducing the intensity and “bending the curve” towards the steps needed to “get to zero”, or from the “three B’s” to the “three C’s”.
The variation in the intensity of disease transmission between localities meant that the shift in strategy was advanced locality by locality, with decisions made based on information – sometimes unverified – from multiple sources. Hence experience sharing and coordination were vital.
Different information sharing mechanisms were used to help groups stay aligned and to appreciate whether there was a need for greater emphasis on the C’s rather than the B’s. They came together in the Global Ebola Response Coalition.
In total, around 10 thousand people died as a result of the 2014 – 15 Ebola outbreak but the spread and damage could have been so much worse had there not been a decision to use systems leadership approaches for directing, coordinating and organizing responses to the outbreak.
There were at least five reviews of action and impact after the Ebola outbreak had calmed down in 2015. The initial learning was situation specific though some entities contributed to more generic lesson-learning.
David Nabarro says: “At the start of this complex assignment I did not know where it would end so I wanted to be sure that however it evolved, we were putting in place ways of working that would be strong enough to last for the duration of the crisis and contribute to an effective response. One of the starting challenges was that different entities, and individuals working for these entities, had very different perceptions of what was going on at any particular point in time, and of what was needed to contain things. Our challenge was to establish conditions in which there was sufficient trust between different entities to encourage them to navigate the differences and sustain the alliance. This meant finding alignment in a rapidly evolving, unstable and undefined environment – it was as much a political as a medical act”.
The vital requirements in this response were a regularly updated strategic direction that reflected the stage of the outbreak, a well-understood organizing framework (the concentration on managing the response in national emergency centres and in local government hubs), and a “big tent” for enabling all concerned to meet at intervals – the GERC.
For establishing the direction of the response, a meaningful narrative was vital. At the beginning the focus was on reducing the overall load of infection to a point where it was possible to know how each person with Ebola became infected. Then it would be possible to move to the next stage where different chains of transmission were contained, and the outbreak curve could be bent to zero.
For the response system, the organizing framework consisted of a) the high-level presence in UNMEER, b) the National emergency response teams – strongly focused on coordination – in each national capital, with a senior officer from UNMEER alongside the national government’s incident manager, and c) the local authority-based coordination at District-level. The US was the primary contributor to Liberia; UK was the primary contributor in Sierra Leone and France was the primary contributor in Guinea.
The big tent was the GERC which offered opportunities for networked leadership and for encouraging alignment despite the large numbers of entities involved in the response.
It is helpful to establish the equivalent of a big tent in which all are welcome. This is often not done because of a sense that a system for expert command and control is key. The problem then is that whoever establishes the tent likes to limit participation to make the proceedings more manageable.
Because a large number of entities were involved in the response, and these reported to different governments and international organizations, a voluntary co-ordination approach was used. It was light touch. In this situation, co-ordination was provided by the UN system and it was made possible through David Nabarro being given authority to do so by the UN Secretary-General. This arrangement for adaptable strategic coordination continued into 2015.
| Acronym | Description |
|---|---|
| GERC | Global Ebola Response Coalition |
| GOARN | Global Outbreak Alert, Action and Response Network |
| NGO | Non-Governmental Organisation |
| UK | United Kingdom |
| UN | United Nations |
| UN S-G | United Nations Secretary General |
| UNICEF | United Nations Children’s Fund |
| UNMEER | UN Mission for Emergency Ebola Response |
| USA | United States of America |
| WHO | World Health Organization |
| WFP | World Food Program |
We gratefully acknowledge the United Nations for entrusting David Nabarro with the responsibility of UN Secretary-General’s Special Envoy on Ebola. We thank all partners, collaborators, and participants who engaged with us throughout this important process.
The views and lessons presented in this paper reflect the experiences and reflections of 4SD’s team. They do not necessarily represent the official views, positions, or endorsements of the United Nations or its affiliated entities.
© 2025 4SD. All rights reserved.
Copyright © 2023 4SD Foundation. All Rights Reserved.
4SD Foundation, Maison Internationale de l’Environnement II, Chemin de Balexert 7-9
1219 Geneva, Switzerland.
With generous support from:

Copyright © 2023 4SD Foundation. All Rights Reserved.
4SD Foundation, Maison Internationale de l’Environnement II, Chemin de Balexert 7-9
1219 Geneva, Switzerland.
With generous support from: